When Neurodegenerative Care Reaches Its Limits, PRISM Extends What’s Possible
Aligned with AAN guidelines—PRISM activates only when functional decline continues despite optimized neurological therapy.
Learn how PRISM supports advanced neurological decline.
➲ Neurological guidelines define the standard of care in degenerative and progressive neurologic conditions.
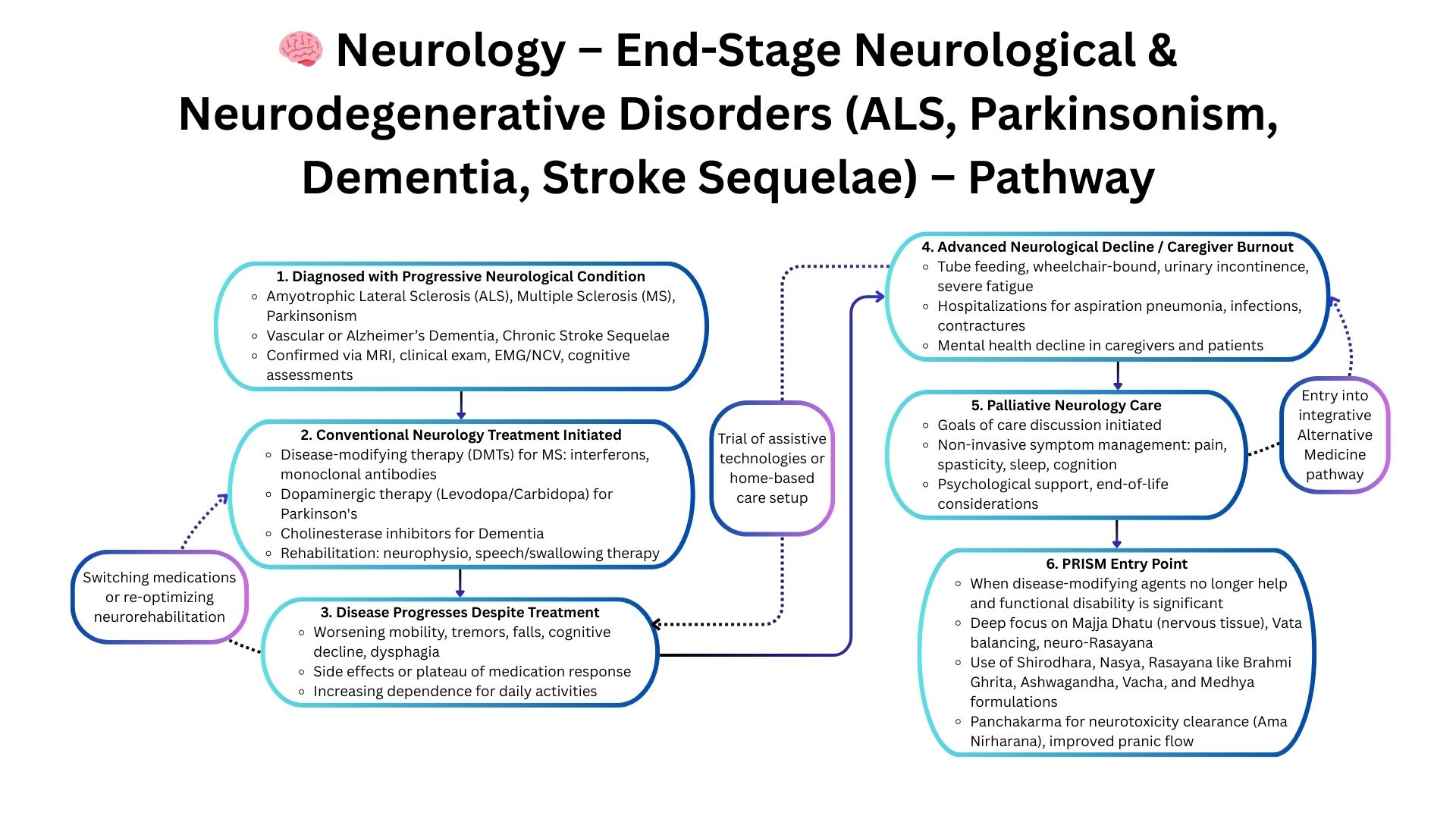
➲ PRISM does not replace these frameworks. It becomes relevant only when functional capacity deteriorates despite dopaminergic therapy, cholinesterase inhibitors, or multidisciplinary neurorehabilitation.
➲ As clinicians consider supportive neurology or palliative pathways, PRISM identifies systemic contributors to decline—stabilizing progression and restoring meaningful function where conventional approaches reach their limit.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
Standard Neurology Care Provides Stability — But Only Up to a Point
Guideline-directed neurological care focuses on disease-modifying therapies, symptom control, rehabilitation, dopaminergic strategies, spasticity management, and supportive care planning. While this stabilizes early and mid-stage disease, a subset of patients continue to decline despite optimized therapy — entering a progressive, multi-system stage where conventional escalation no longer alters the trajectory.
In advanced neurological conditions, deeper system-level drivers accelerate deterioration:
- Neuro-degenerative metabolic failure
- Autonomic dysfunction affecting sleep, BP, HRV
- Mitochondrial exhaustion impairing motor recovery
- Neuro-immune activation fueling chronic progression
- Microbiome–neuro interactions influencing symptoms
- Phenotype patterns predicting speed of decline
These systemic mechanisms are not addressed in standard neurological guidelines, which rely heavily on pharmacological escalation or device-based interventions.
Where Traditional Approaches Fall Short
Progressive decline despite optimal therapy
Conditions like ALS/MND, advanced Parkinson’s, and progressive MS continue deteriorating even when guideline-recommended therapy is maximized.
Multi-domain neurological failure
Motor, cognitive, autonomic, sleep, and metabolic domains fail together — but standard pathways address them separately, missing the interconnected drivers.
Limited escalation options
When DBS, pump therapy, biologics, or disease-modifiers are no longer feasible or effective, guidelines offer no next step — despite ongoing clinical decline.
PRISM: A Systems-Driven Framework for Advanced Neurology
Why PRISM Works When Neurology Guidelines Stop
PRISM identifies the systemic drivers accelerating neurological deterioration:
- Neuro-immune activation driving progression
- Mitochondrial dysfunction limiting neuronal resilience
- Autonomic imbalance detected through HRV, sleep, BP variability
- Gut–neuro axis disturbances influencing inflammation & symptom cycles
- Metabolic rigidity worsening fatigue and motor decline
- Phenotype mapping that predicts which systems fail first
This multi-layered understanding allows clinicians to manage advanced neurological conditions more predictively, improving stability, functional maintenance, and symptom control even when guideline-based escalation has reached its limit.