When Guideline-Directed Heart Failure Therapy Reaches Its Limits, PRISM Extends What’s Possible
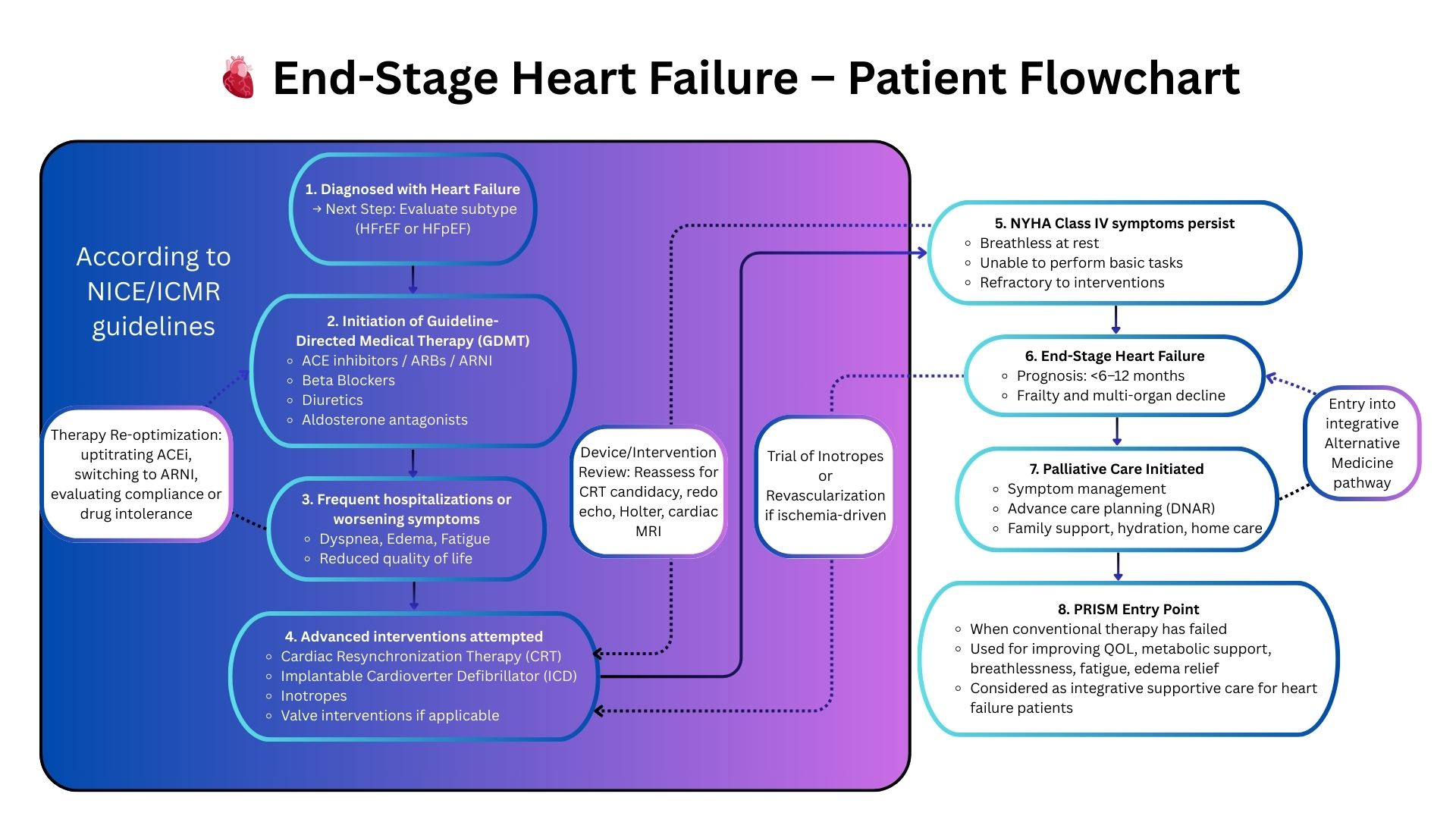
Aligned with ACC/AHA guidelines and global cardiology standards—PRISM becomes relevant only when heart failure progresses despite optimal GDMT.
Discover PRISM’s impact in advanced heart failure.
➲ Clinical guidelines for heart failure represent the pinnacle of evidence-based cardiology.
➲ PRISM does not replace these sacrosanct pathways. It becomes clinically meaningful only when the patient remains symptomatic, deteriorating, or refractory to quadruple therapy, device optimization, and advanced interventions.
➲ When the conversation shifts toward palliative heart failure care or limited supportive trajectories, PRISM adds a systems-medicine layer that uncovers hidden contributors, stabilizes decline, and meaningfully improves function—supporting, not opposing, guideline-directed care.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
Standard Cardiology Care Works — But Only Up to a Point
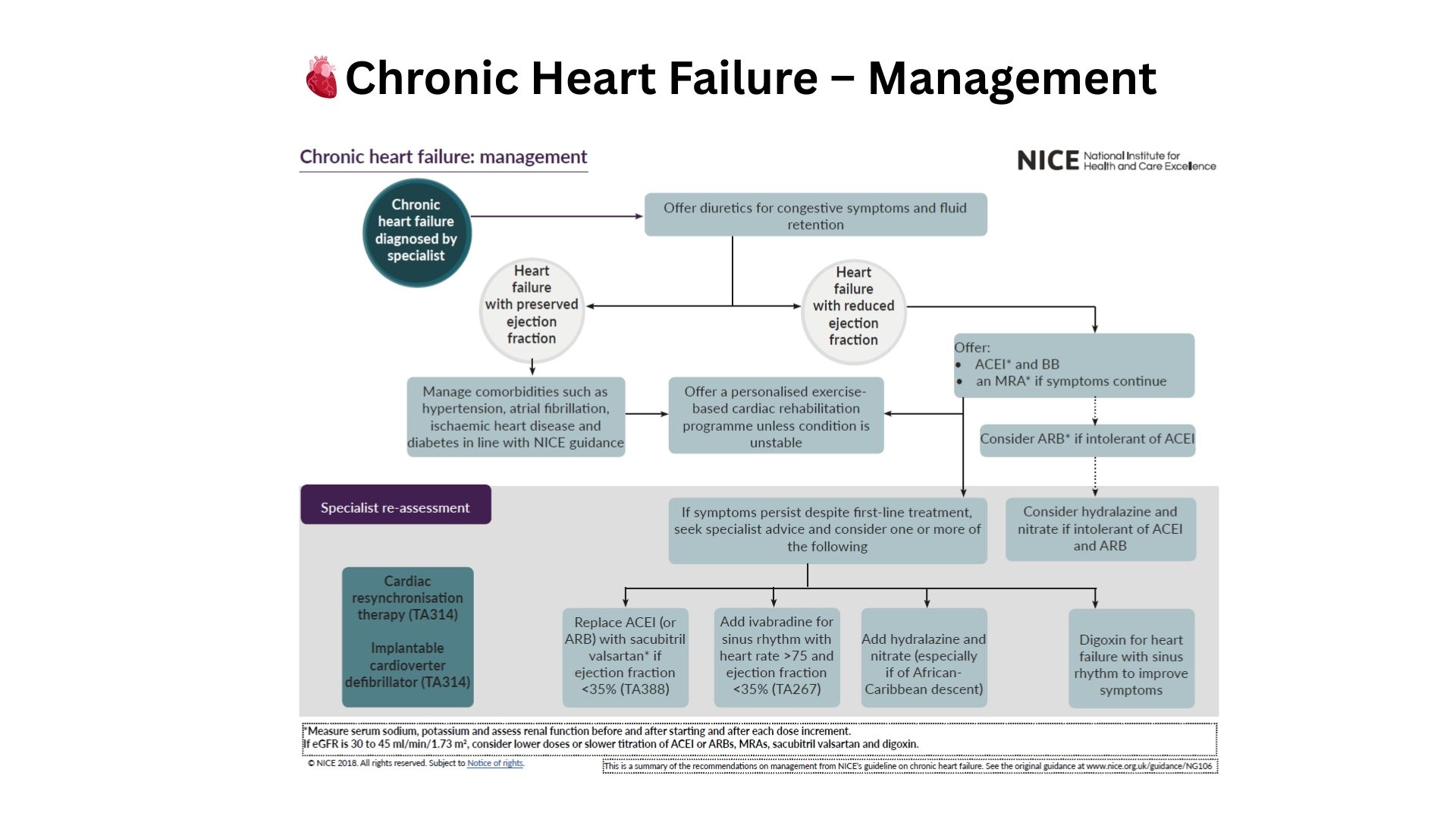
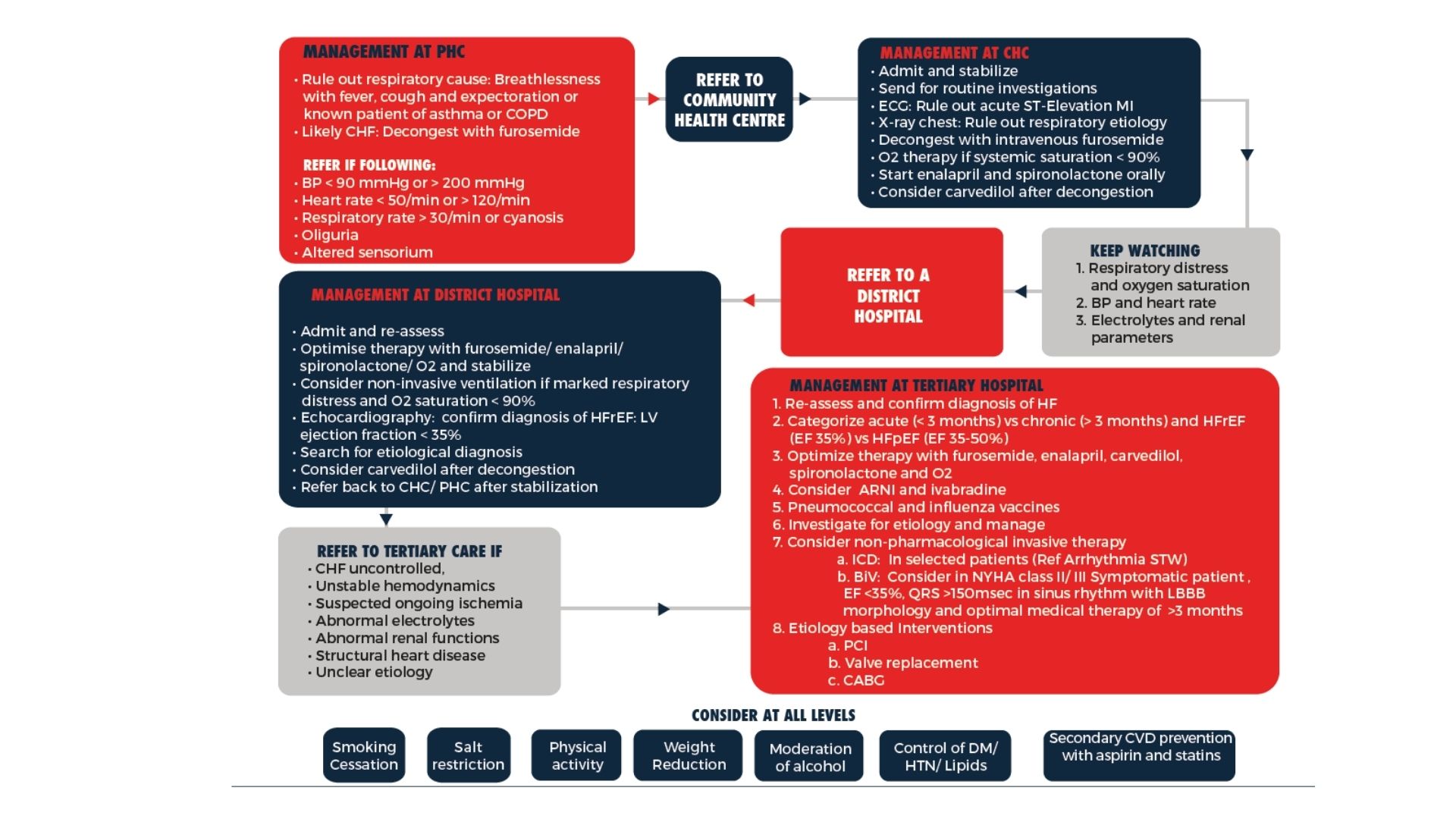
Guideline-directed cardiac therapy (ICMR/NICE) focuses on GDMT escalation, revascularization decisions, rhythm management, and device eligibility. For many patients this provides stability — but once cardiac disease becomes refractory or progresses into multi-system decline, a purely organ-centric model is no longer enough.
In advanced heart failure and complex cardiac conditions, deeper drivers influence disease progression:
- Neuro-hormonal overactivation
- Autonomic imbalance (vagal withdrawal, low HRV)
- Inflammatory & immune dysregulation
- Metabolic impairment and mitochondrial stress
- Cardio-renal & cardio-hepatic interactions
- Phenotype-specific patterns affecting prognosis
These systemic contributors fall outside standard guideline algorithms, which focus on medication titration and device-based escalation.
Where Traditional Approaches Fall Short
Progressive Heart Failure Despite GDMT
NYHA-IV patients or those with repeated admissions continue to worsen even when guideline medications are optimized.
Multi-system Cardiac Interactions
Cardio-renal syndrome, hepatic congestion, frailty, and inflammatory states complicate care — factors traditional guidelines do not address.
Patients Not Eligible for Interventions
When surgery, PCI, transplant, or VAD are contraindicated, conventional pathways offer very limited forward options.
PRISM: A Systems-Driven Clinical Framework for Cardiology
Why PRISM Works When Guidelines Stop
PRISM augments GDMT by mapping the systems biology behind cardiac decline:
- Neuro-autonomic imbalance influencing rhythm and perfusion
- Inflammatory & immune activation driving HF progression
- Metabolic instability contributing to fatigue and low output states
- Gut-immune interactions impacting inflammation and fluid balance
- Digital markers (HRV, sleep, stress signatures) revealing disease trajectory
- Phenotype mapping to prioritize individualized interventions
This enables clinicians to identify system-level drivers that explain why a patient is deteriorating despite guideline-directed therapy, allowing safer, smarter and more predictive clinical decisions.