When Refractory Allergic or Immune Disease Reaches Its Limits, PRISM Extends What’s Possible
Aligned with AAAAI (American Academy of Allergy, Asthma & Immunology), EAACI (European Academy of Allergy & Clinical Immunology), and global immunology guidelines—PRISM activates only when inflammation, airway obstruction, or immune instability persist despite optimized evidence-based therapy.
Learn how PRISM supports complex allergic and immune disorders.
➲ Guideline-directed allergology & immunology form the core of care—from stepwise asthma escalation, biologics, immunotherapy, and immune-modulating protocols.
➲ PRISM does not replace these standards. It becomes relevant only when severe asthma, immune dysfunction, or inflammatory disease persists despite maximal recommended therapy.
➲ When clinicians consider non-biologic pathways, non-escalation routes, or supportive immune stabilization, PRISM uncovers deeper systemic contributors—gut–immune imbalance, autonomic dysregulation, metabolic stress, inflammatory cycles, and phenotype patterns—helping stabilize symptoms, reduce flares, and strengthen resilience.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
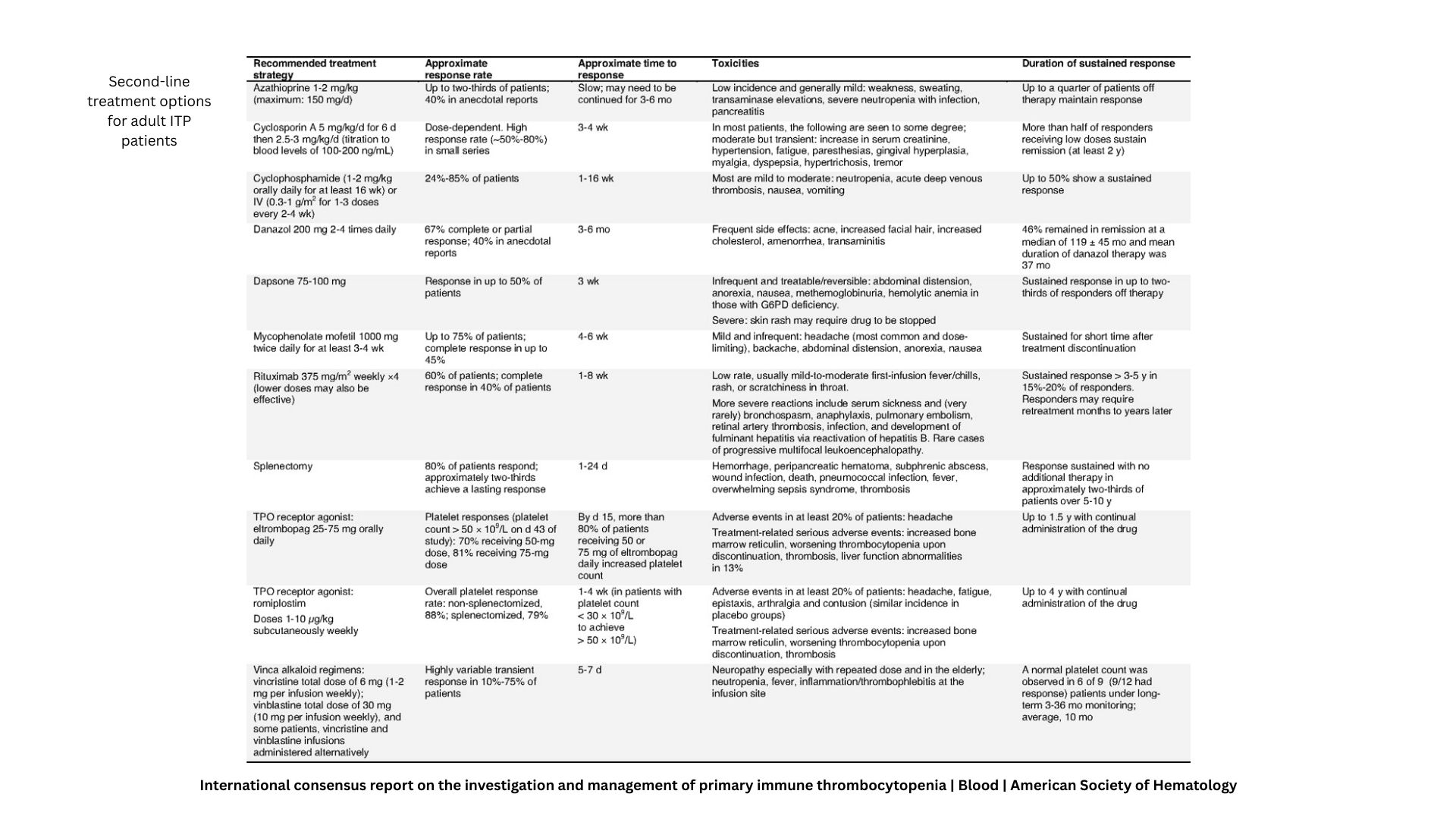
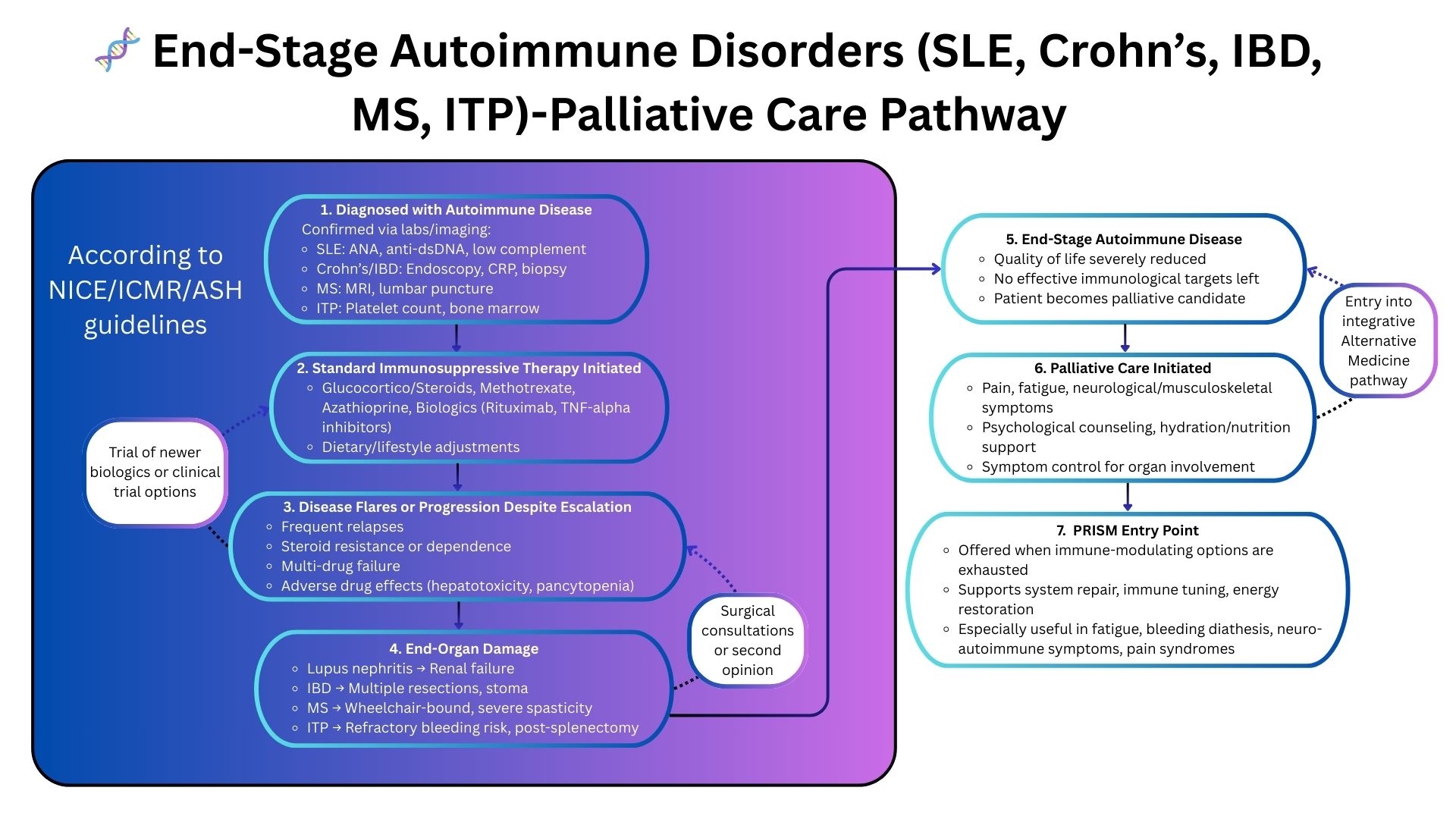
Standard Autoimmune Care Works — But Only Up to a Point
Guideline-directed autoimmune management focuses on immunosuppressants, biologics, steroid protocols, and organ-preservation strategies. While many patients stabilize, a significant subset continues to progress despite optimal therapy — entering a phase where inflammation becomes systemic, multi-organ, and resistant to escalation.
In refractory autoimmune disease, deeper system-level drivers sustain the cycle:
- Immune hyperactivation with cytokine persistence
- Loss of immunological tolerance
- Microbiome–immune dysregulation fueling flares
- Mitochondrial stress & metabolic exhaustion
- Neuro-immune interactions influencing symptom cycling
- Phenotype-specific flare patterns that alter prognosis
These systemic contributors lie outside standard guideline algorithms, which depend largely on escalating immunosuppression.
Where Traditional Approaches Fall Short
Refractory disease despite escalation
Conditions like SLE, vasculitis, and systemic sclerosis continue to progress even after steroids, DMARDs, or biologics are maximized.
Multi-organ involvement with no remaining options
Renal, pulmonary, neurological, and skin complications often evolve simultaneously, overwhelming organ-specific treatment pathways.
High toxicity or non-response to therapy
Many patients cannot tolerate further immunosuppression due to infections, cytopenias, or organ damage — leaving no guideline-based alternatives.
PRISM: A Systems-Driven Clinical Framework for Autoimmune Disease
Why PRISM Works When Guidelines Stop
PRISM uncovers the system-level mechanisms fueling autoimmune progression:
- Immune-metabolic imbalance sustaining chronic inflammation
- Neuro-immune dysregulation affecting flare frequency
- Gut-immune interactions driving systemic autoimmunity
- Mitochondrial dysfunction reducing healing and recovery
- Digital markers (HRV, sleep, stress) revealing instability before flare
- Phenotype mapping identifying which pathways dominate the illness
This enables clinicians to identify why the patient is deteriorating despite guideline-directed therapy — allowing individualized and safer system-guided interventions.