When Guideline-Directed COPD or ILD Care Reaches Its Limits, PRISM Extends What’s Possible
Respecting GOLD, ATS, and ERS standards—PRISM activates only when respiratory decline persists despite maximal guideline-based therapy.
See how PRISM supports care in advanced respiratory disease.
➲ Guideline-directed therapy is central to managing COPD, ILD, and progressive lung disease.
➲ PRISM does not replace these evidence-backed protocols. It becomes relevant only when the patient continues to decline despite bronchodilator escalation, anti-fibrotics, pulmonary rehabilitation, or long-term oxygen therapy.
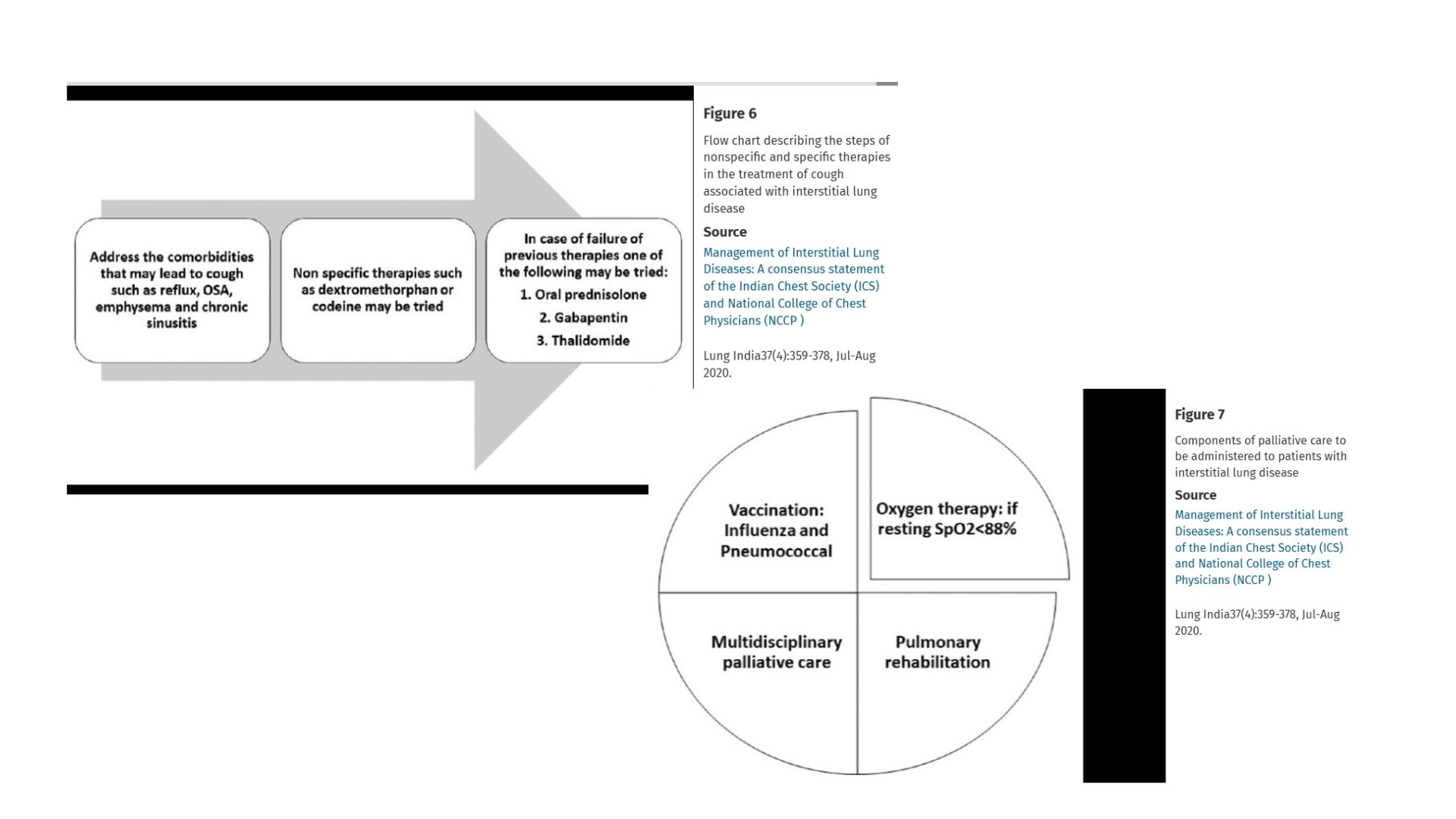
➲ When clinicians begin discussing palliative pulmonology or end-stage supportive care, PRISM introduces a systems-medicine perspective that stabilizes deterioration, uncovers reversible contributors, and restores meaningful function.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
Standard Pulmonology Works — Until the Disease Becomes Refractory
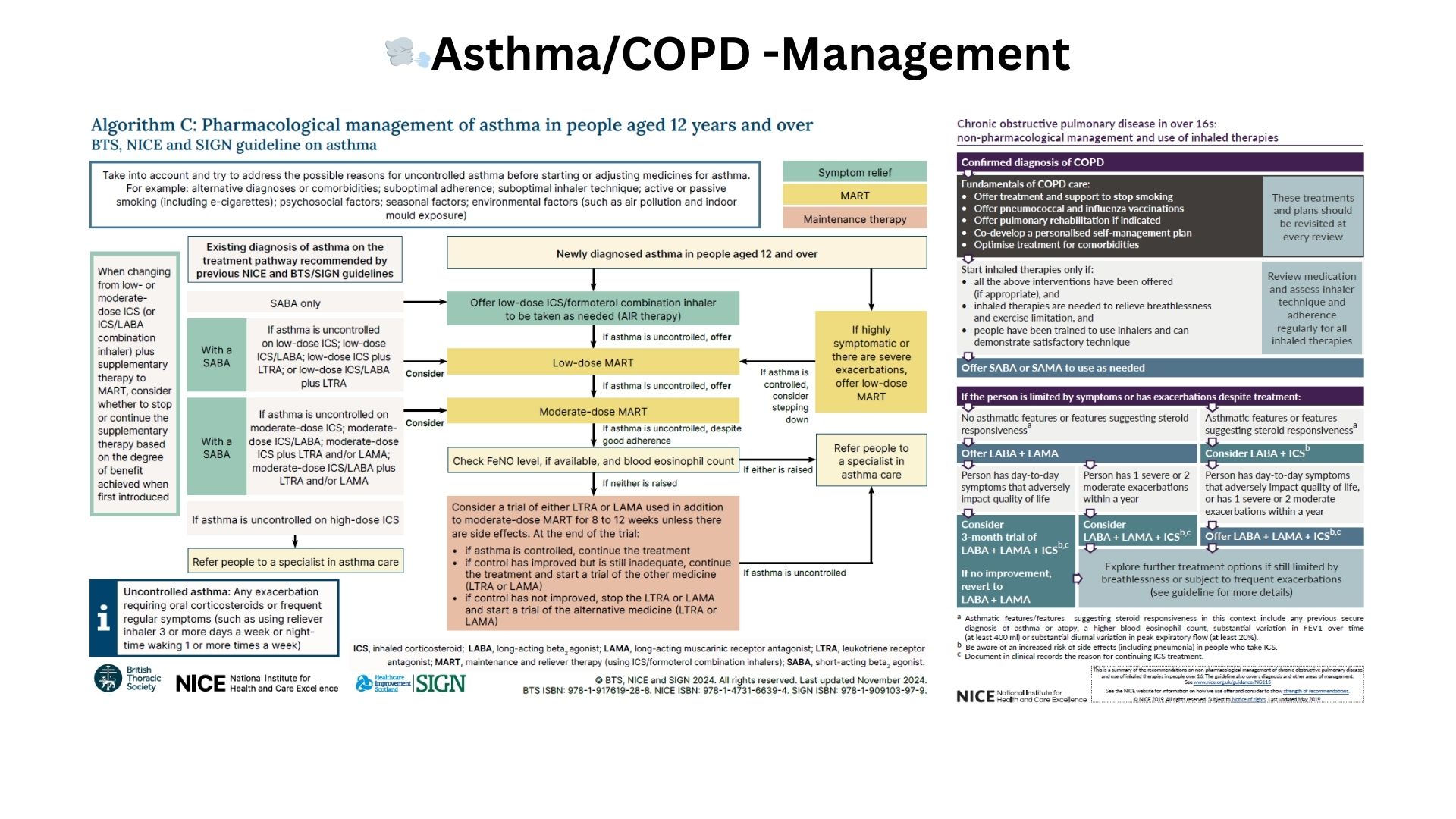
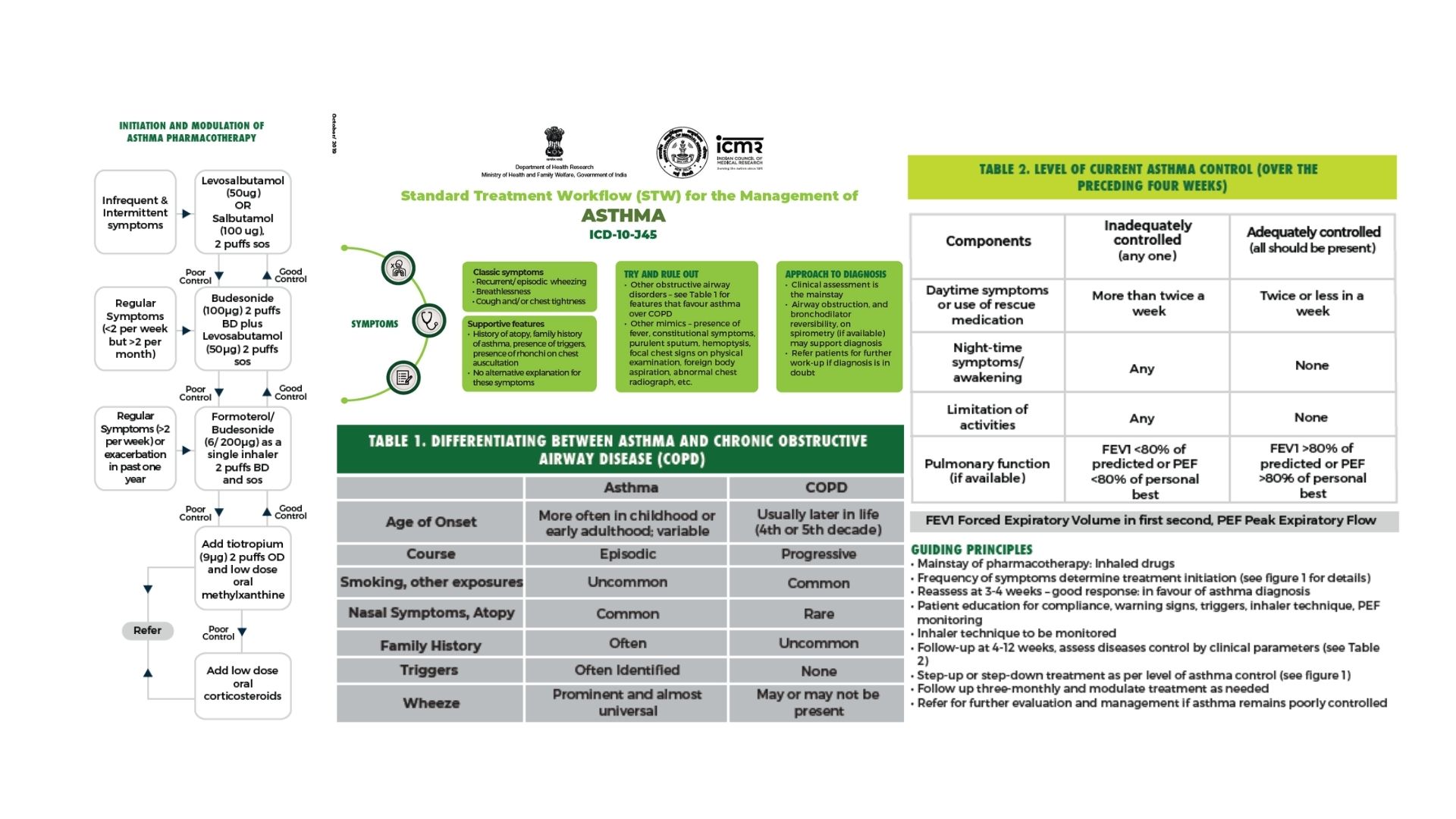
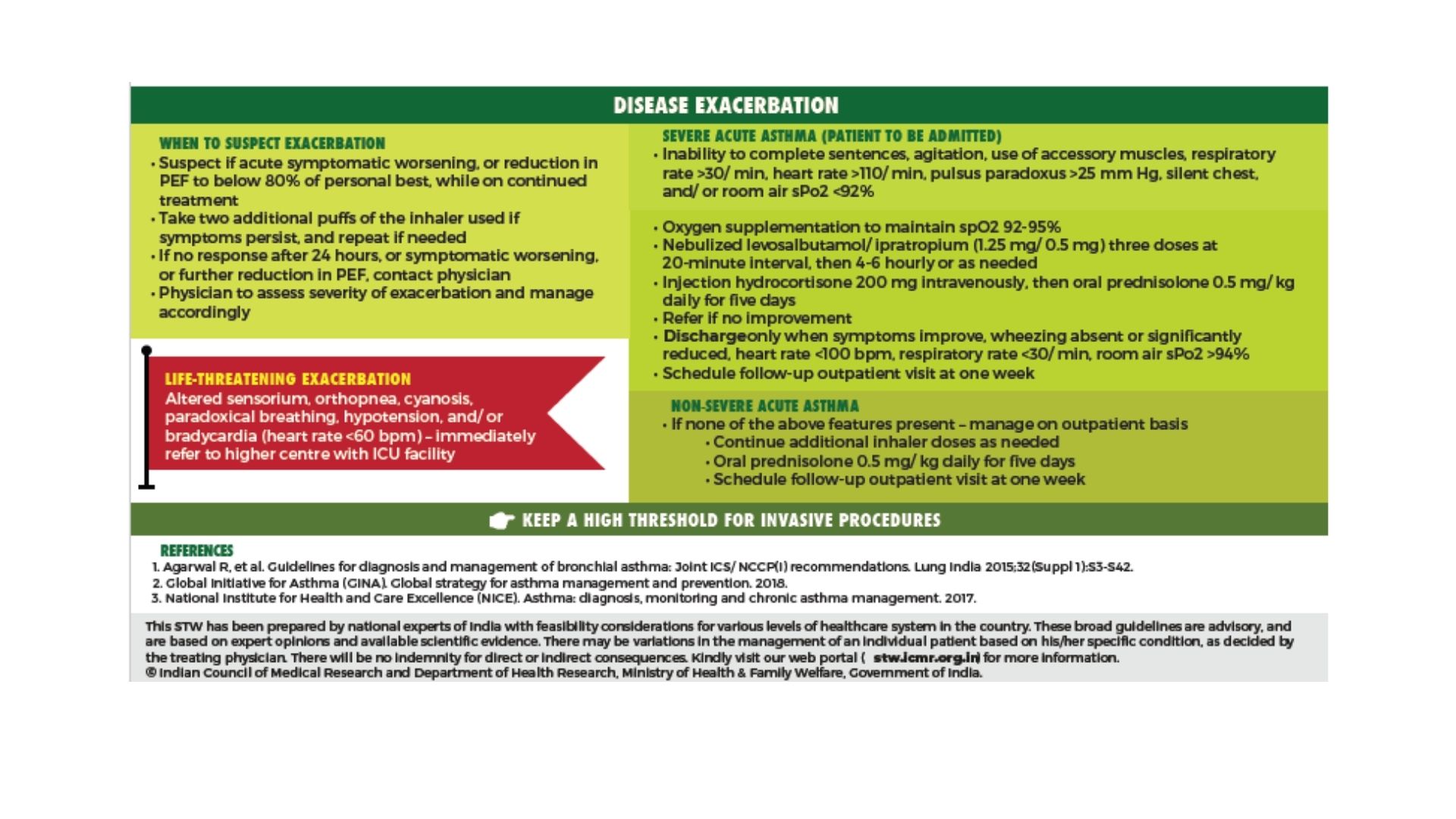
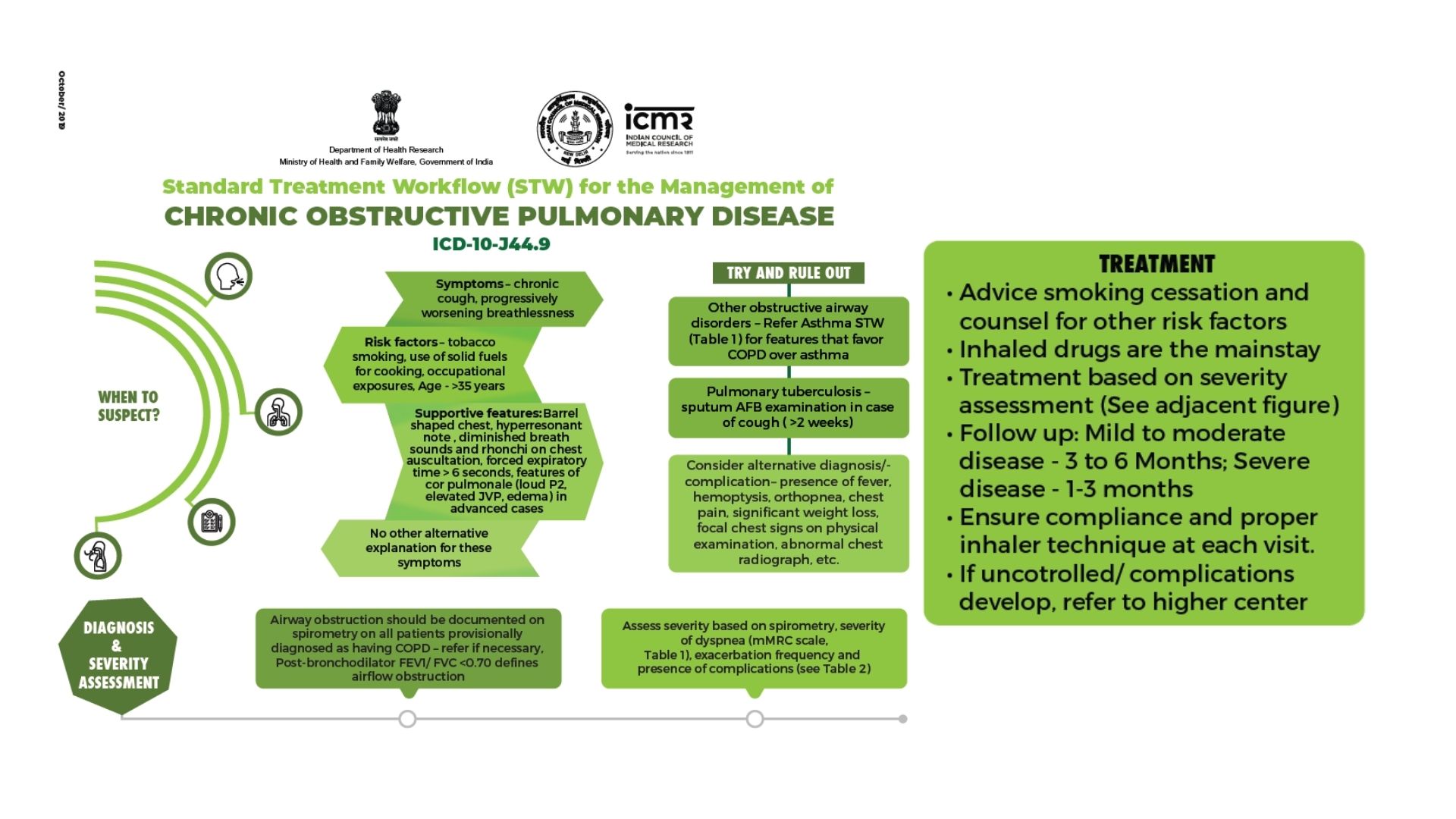
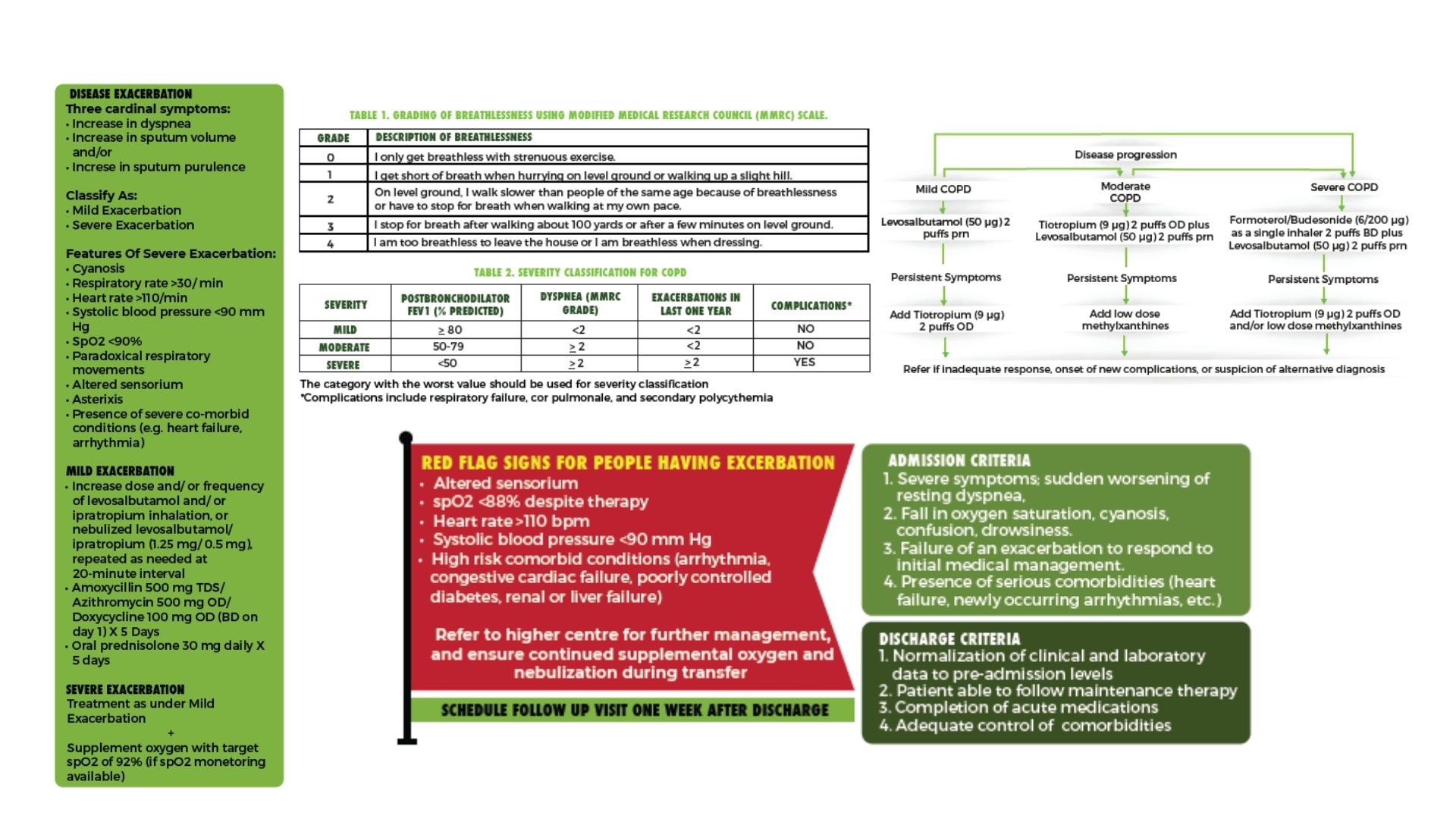
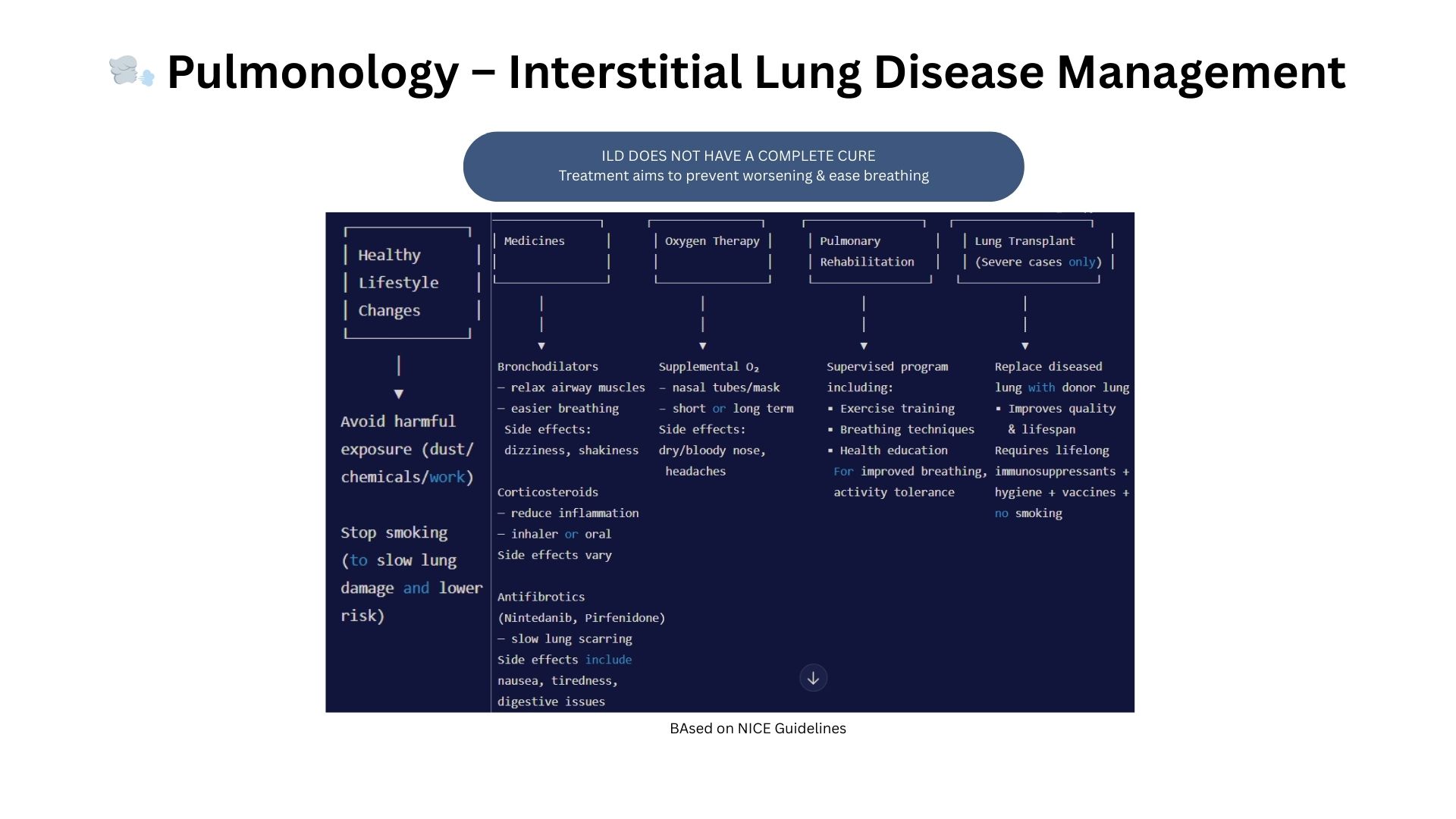
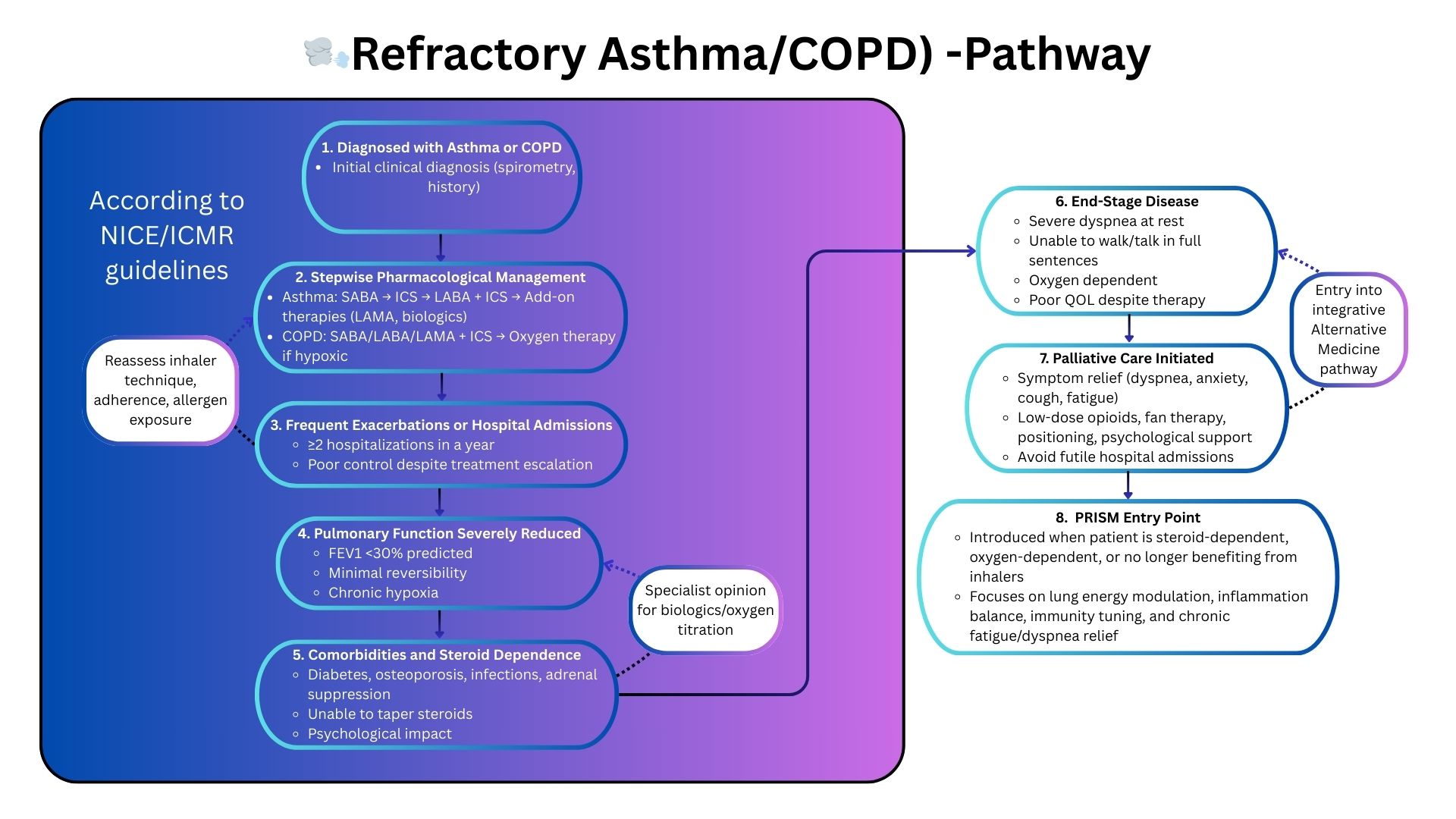
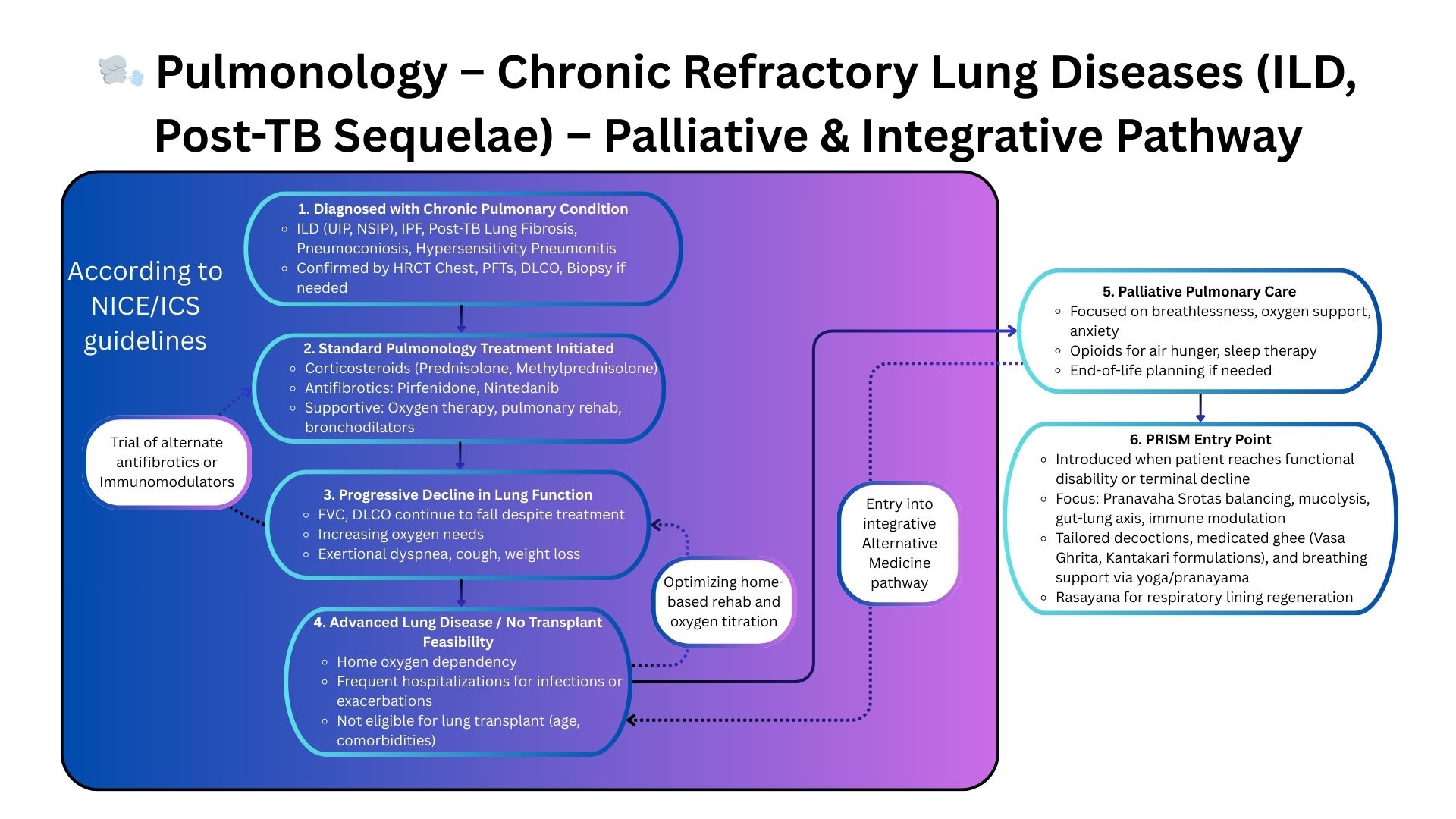
Pulmonology guidelines (ICMR/NICE/GINA/GOLD) provide clear escalation pathways: bronchodilators, inhaled steroids, biologics for asthma, antifibrotics, pulmonary rehab, oxygen therapy, and interventional options.
While highly effective in early and moderate disease, these pathways begin to fail when patients enter steroid-refractory asthma, progressive interstitial lung disease, advanced COPD with fixed airflow limitation, or severe bronchiectasis despite maximal therapy.
The true drivers of deterioration at this stage are not airway mechanics alone, but multi-system dysfunction:
- Immune hyperreactivity sustaining airway inflammation
- Chronic low-grade systemic inflammation worsening fatigue and symptoms
- Gut–lung axis imbalance influencing flares and exacerbation frequency
- Autonomic dysregulation affecting breathlessness and sleep
- Mitochondrial fatigue impairing recovery and exercise tolerance
- Phenotype patterns determining disease behavior and response
These deeper layers remain outside the scope of traditional pulmonology guidelines, leaving clinicians with limited options once standard escalation plateaus.
Where Traditional Pulmonology Falls Short
Steroid-refractory / biologic-refractory asthma
Flares, fixed obstruction, or eosinophilic activity persist despite maximal biologics or steroid therapy.
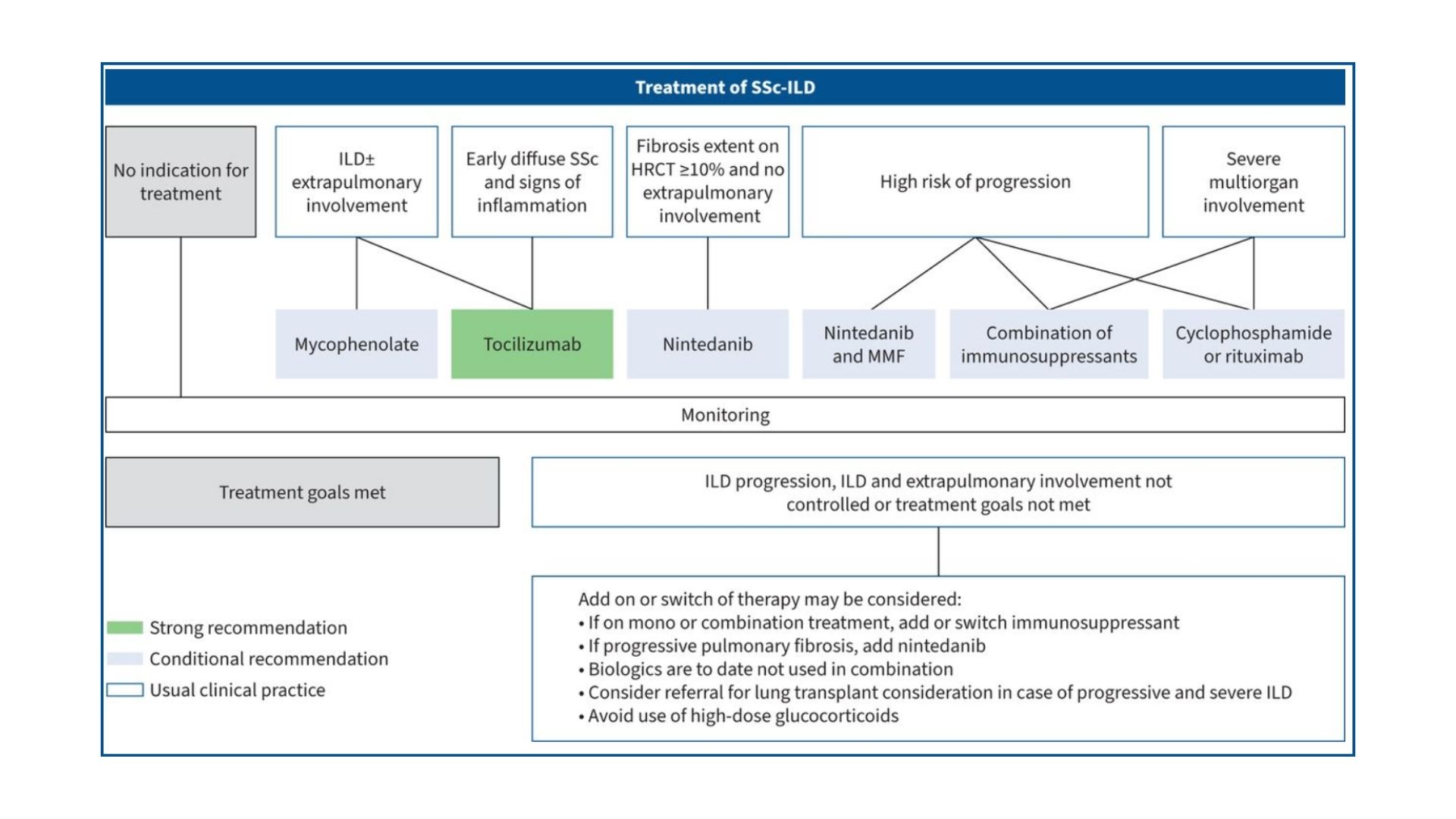
Progressive ILD or COPD despite guideline care
Decline continues even with antifibrotics, oxygen therapy, and pulmonary rehabilitation.
Multi-system complexity
Breathlessness, fatigue, cachexia, dysbiosis, sleep disturbance, and autonomic instability cannot be explained by lung pathology alone.
PRISM: A Systems Medicine Framework for Complex Pulmonary Disease
Why PRISM Helps When Pulmonology Guidelines Reach Their Limit
PRISM evaluates systemic factors that determine pulmonary outcomes:
- Immune–inflammatory loops driving persistent airway hyperreactivity
- Gut–lung axis dysfunction increasing exacerbations
- Autonomic dysregulation worsening dyspnea and sleep
- Mitochondrial failure limiting exercise capacity
- Metabolic instability enhancing fatigue and steroid sensitivity
- Digital markers (HRV, sleep, exertion signatures) revealing hidden instability
- Phenotype-guided mapping for personalized intervention pathways
PRISM helps stabilize symptoms, reduce flare frequency, enhance functional capacity, slow disease progression, and improve quality of life — especially in patients who are not responding to standard pulmonology pathways.