When CKD or ESRD Management Reaches Its Limits, PRISM Extends What’s Possible
Honoring KDIGO and nephrology guidelines—PRISM activates only when decline persists despite maximal medical therapy.
Learn how PRISM supports advanced kidney disease.
➲ Guidelines define the backbone of CKD and ESRD management.
➲ PRISM does not replace them. It becomes relevant only when renal decline continues despite optimization of blood pressure, metabolic parameters, and renal-protective therapy.
➲ When clinicians begin discussing dialysis dependence, palliative nephrology, or supportive-only pathways, PRISM identifies systemic imbalances that may still be modifiable—improving stability, function, and quality of life even near end-stage.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
Guideline-Based Nephrology Works — Until the Disease Outgrows It
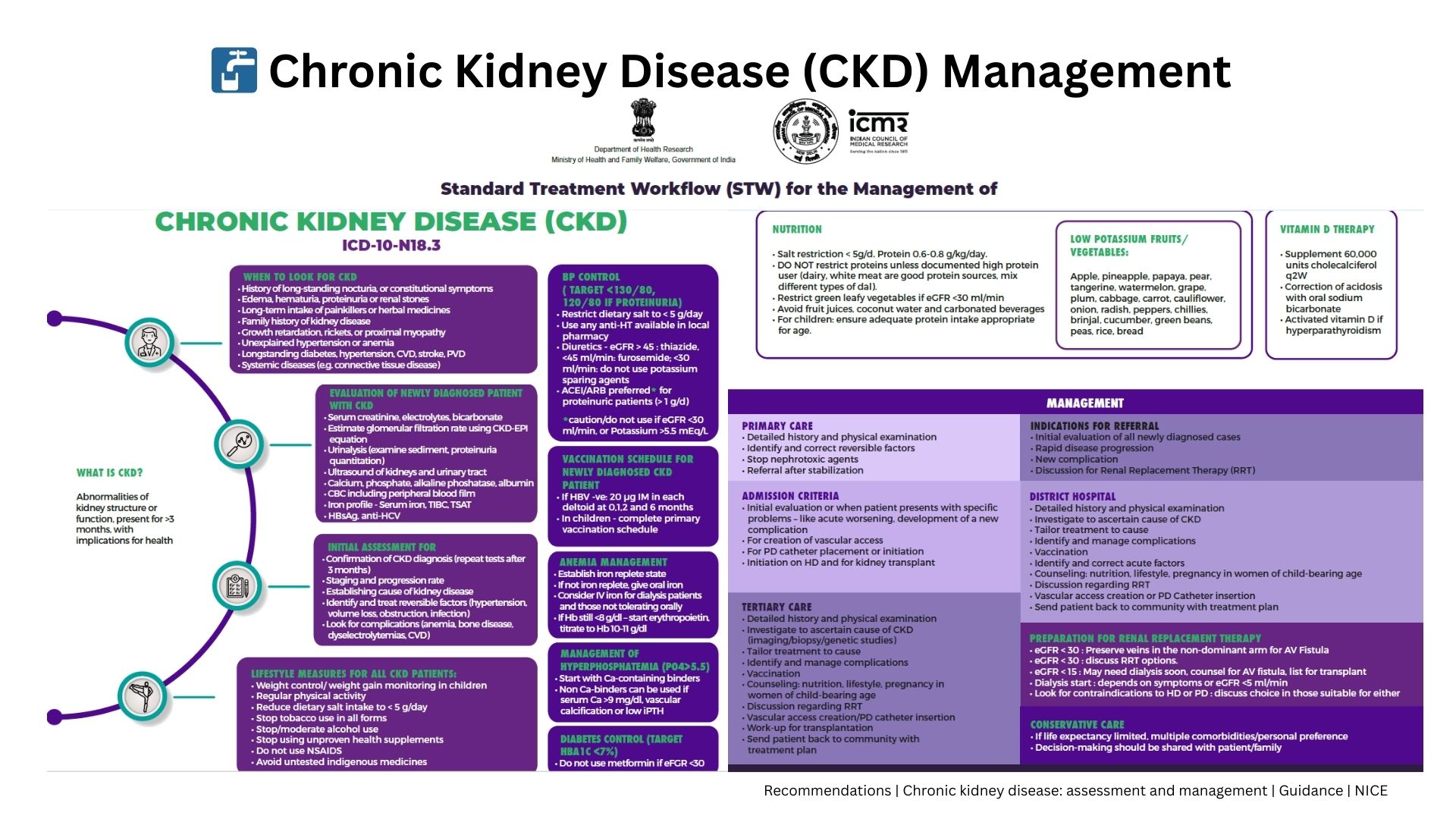
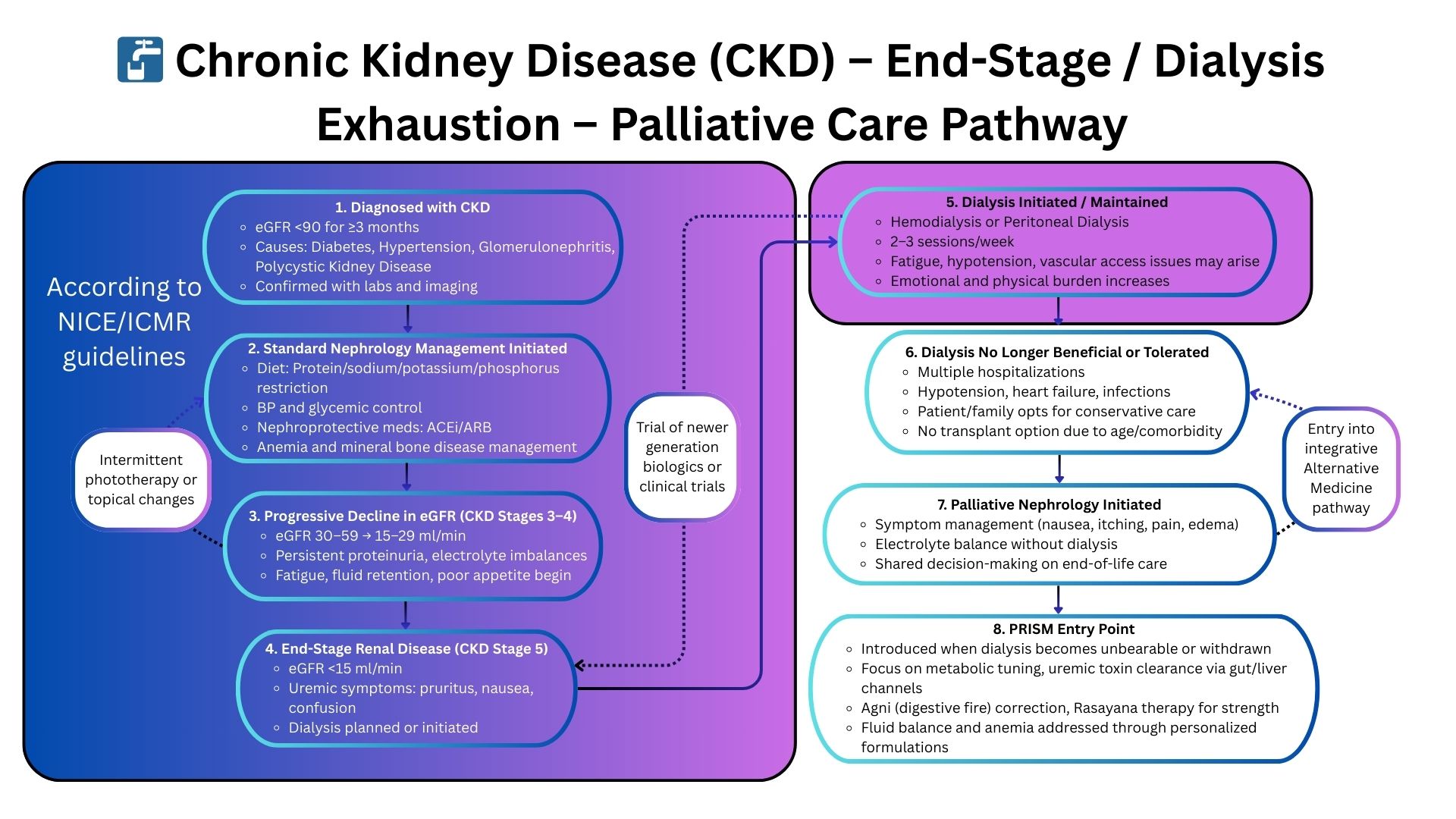
Standard kidney-care pathways (ICMR/NICE) focus on slowing CKD progression, managing electrolytes, optimizing BP, correcting anemia, and preparing patients for dialysis or transplant when needed.
While effective for early and mid-stage CKD, these pathways begin to fail when patients enter: ESRD without dialysis options, progressive CKD with cachexia, refractory metabolic symptoms, or recurring hospitalizations despite guideline therapy.
At this point, renal decline is no longer driven by GFR alone. It stems from deeper, multi-system dysfunction:
- Chronic inflammation and immune activation accelerating organ loss
- Gut–kidney axis disruption increasing uremic toxin burden
- Metabolic acidosis driving catabolism and frailty
- Autonomic dysregulation worsening BP and fluid instability
- Mitochondrial failure leading to low energy and cachexia
- Phenotypic and constitutional patterns shaping symptom severity
These drivers sit outside the scope of traditional nephrology guidelines — leaving clinicians with limited tools once standard pathways are exhausted.
Where Traditional Nephrology Falls Short
ESRD progression in non-dialysis candidates
Frail or multi-morbid patients who cannot undergo dialysis experience accelerating decline despite optimal medical therapy.
Systemic instability not explained by kidney numbers
Fluid overload, metabolic acidosis, neuropathy, and sleep disturbance arise from whole-body dysfunction, not GFR alone.
High symptom burden despite guideline-directed therapy
Patients often feel worse than their labs suggest — reflecting invisible autonomic, inflammatory, and metabolic drivers.
PRISM: A Systems Medicine Approach to Advanced Renal Disease
Why PRISM Succeeds When Nephrology Guidelines Reach Their Limit
PRISM identifies and corrects the systemic drivers accelerating CKD and ESRD:
- Gut–kidney axis inflammation and toxin accumulation
- Autonomic imbalance affecting BP, fatigue, and fluid shifts
- Metabolic acidosis fueling inflammation and muscle breakdown
- Mitochondrial energy failure worsening frailty
- Immune dysregulation influencing progression and symptoms
- Phenotype-specific disease patterns guiding personalized care
- Digital markers (HRV, sleep, stress) revealing hidden instability
This whole-system mapping enables clinicians to stabilize complex renal cases, reduce hospitalizations, improve energy, slow functional decline, and enhance quality of life — especially when dialysis or transplant are not options.