When End-Stage Liver Disease Management Reaches Its Limits, PRISM Extends What’s Possible
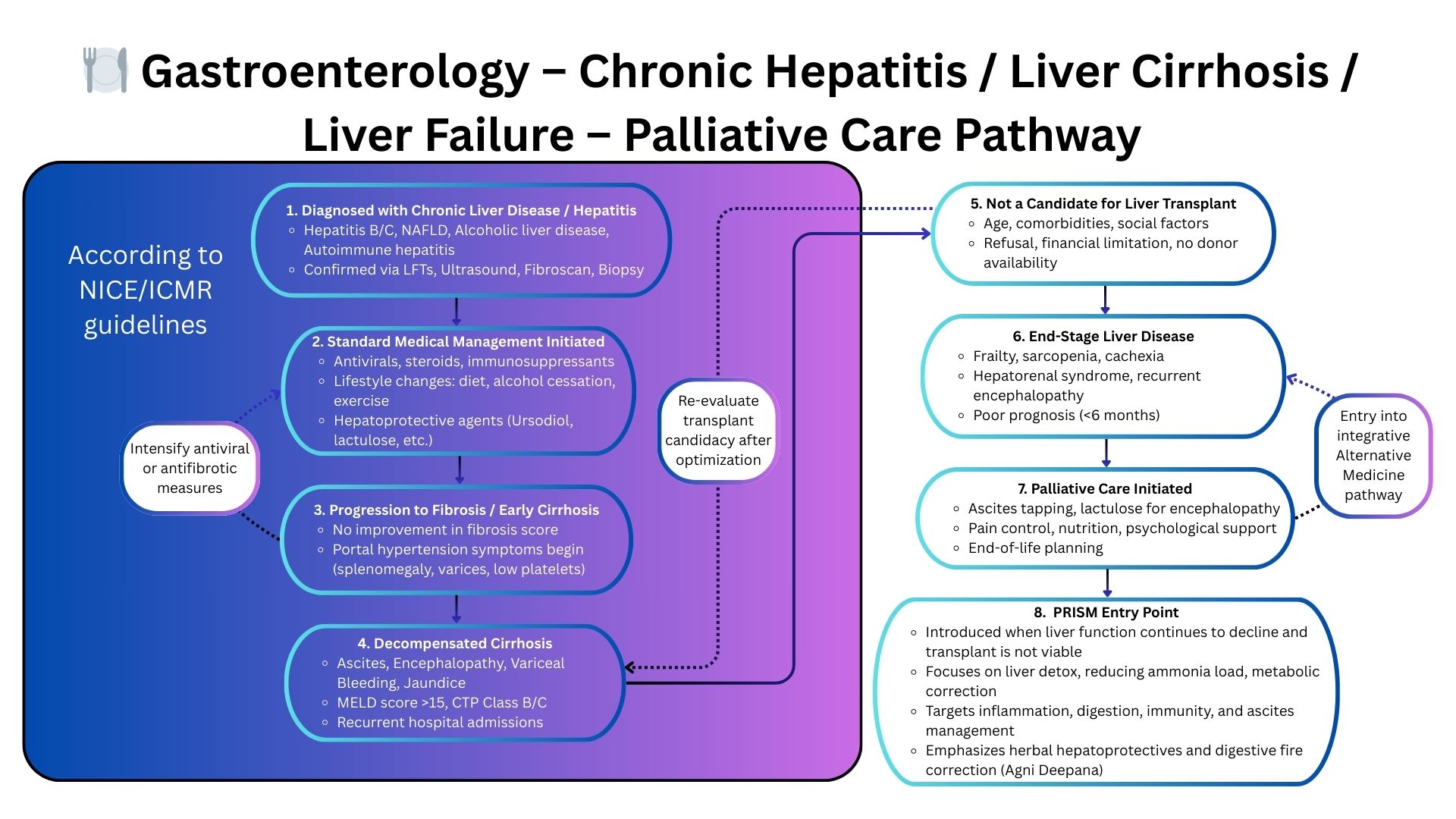
Aligned with AASLD and global hepatology guidelines—PRISM activates only when decompensation persists despite optimized medical and supportive therapy.
Learn how PRISM supports advanced liver disease.
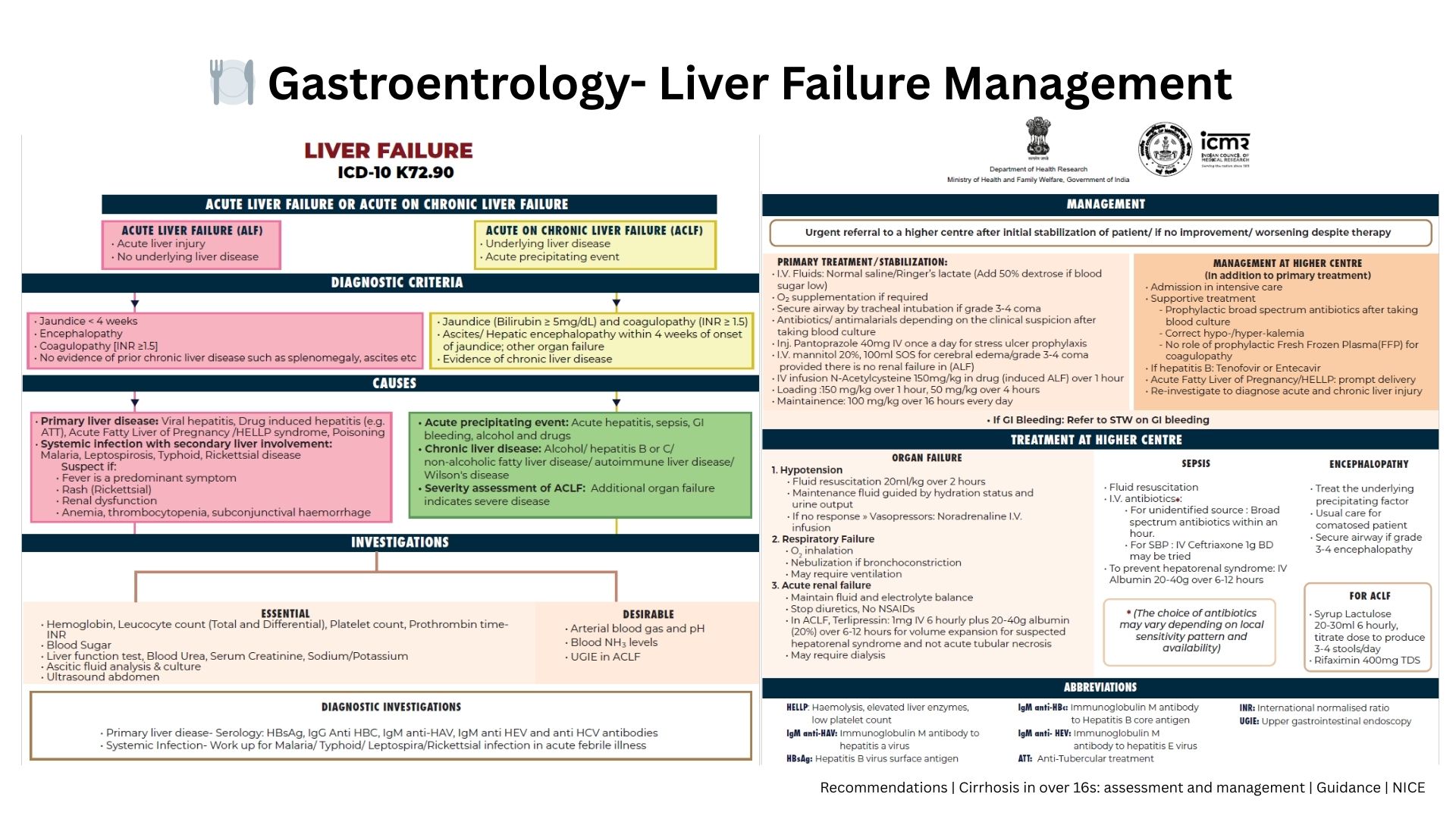
➲ Evidence-based hepatology guidelines shape every therapeutic decision in chronic and end-stage liver disease.
➲ PRISM does not replace them. It becomes relevant only when ascites, encephalopathy, or systemic instability persist despite maximum recommended management.
➲ When clinicians consider transplant-ineligible pathways or supportive hepatology care, PRISM uncovers hidden systemic imbalances and stabilizing opportunities—enhancing function, reducing decline, and improving overall resilience.
From Guidelines to Systems Thinking: Why PRISM Changes the Clinical Outcome
Standard Gastroenterology Care Works — Until Disease Becomes Systemic
Traditional gastroenterology guidelines prioritize structural and organ-directed treatment: endoscopy-based interventions, immunosuppressive escalation for IBD, portal pressure control in cirrhosis, nutritional correction, and pain management protocols.
These approaches are essential, but for patients with decompensated cirrhosis not eligible for transplant, refractory Crohn’s/IBD with irreversible decline, or chronic pancreatitis with malnutrition and unrelenting pain — guideline pathways eventually reach a limit.
In these late-stage conditions, progression is often driven by deeper systemic processes that guidelines do not address:
- Chronic inflammatory loops sustaining gut injury
- Gut–immune axis dysregulation
- Microbiome malfunction affecting liver and bowel disease
- Neuro-visceral imbalance driving pain + motility issues
- Metabolic and mitochondrial impairment worsening fatigue and frailty
- Phenotype-driven vulnerability patterns influencing disease expression
These overlooked layers explain why some patients worsen even with optimal guideline-directed therapy.
Where Traditional Approaches Fall Short
Decompensated cirrhosis without transplant options
Portal hypertension, sarcopenia, ascites, and hepatic encephalopathy progress even with maximal medical therapy when transplant is not feasible.
Refractory Crohn’s or IBD with structural decline
Even after biologics, immunosuppression, and surgery, some patients continue to deteriorate — often due to unrecognized immune–gut–metabolic interactions.
Chronic pancreatitis with severe pain + malnutrition
Recurrent inflammation, dysbiosis, neuro-immune sensitization, and metabolic instability drive symptoms long after procedural options are exhausted.
PRISM: A Systems-Biology Framework for Complex Gastrointestinal Disease
Why PRISM Works When GI Guidelines Are No Longer Enough
PRISM addresses the systems that drive progression in late-stage GI disease — going beyond endoscopy, immunosuppression, and nutritional correction to uncover multi-system drivers:
- Gut–immune axis dysfunction sustaining inflammation
- Microbiome collapse affecting liver, bowel, and metabolic pathways
- Neuro-visceral dysregulation driving pain, motility, and hypersensitivity
- Metabolic + mitochondrial stress worsening frailty and fatigue
- Immune-metabolic loops influencing disease severity and relapse cycles
- Phenotype-based stratification for personalized priority setting
Through this lens, PRISM helps clinicians stabilize decline, reduce symptom burden, and improve function in patients who have exhausted guideline-defined GI care pathways.